CRISTIAN SALAZAR C, ALLEN DIAZ I, RICARDO ROJAS D, MIGUEL GAITAN C, ARMANDO LUCAR F.
Tipo:
Case Report
ABSTRACT (English):
Introduction: The complexity of an intracranial aneurysm is defined by its location, size, previous treatment, presence or absence of collateral circulation, intraluminal thrombus, or calcification of the aneurysm wall. The treatment of these aneurysms must be based on the balance between the associated risks and the benefit for the patient; Within microsurgical techniques, the extradural minipterional approach is described.
Clinical case: a 33-year-old female patient who presented headache, vomiting, and sensorial disorder, being diagnosed with 2 complex aneurysms, one in the ruptured ophthalmic segment and the other in the unruptured right pituitary. She underwent an extradural minipterional craniotomy plus aneurysm clipping with complete occlusion and a favorable outcome.
Conclusion: The knowledge of new microsurgical techniques in the management of complex cerebral aneurysms is crucial to obtain satisfactory results, being the extradural minipterional approach an alternative and key approach for the treatment of these lesions, which represent a challenge for the neurosurgeon.
Keywords: Intracranial Aneurysm, Craniotomy, Collateral Circulation, Neurosurgeons (Source: MeSH NLM)
ABSTRACT (Spanish):
Introducción: La complejidad de un aneurisma intracraneal está definido por su ubicación, tamaño, tratamiento previo, presencia o ausencia de circulación colateral, trombo intraluminal o calcificación de la pared del aneurisma. El tratamiento de estos aneurismas debe basarse en el equilibrio entre los riesgos asociados y el beneficio para el paciente; dentro de las técnicas microquirúrgicas se describe el abordaje minipterional extradural.
Caso clínico: Paciente mujer de 33 años que presentó cefalea, vómitos y trastorno del sensorio, siendo diagnosticada de 2 aneurismas complejos, uno en el segmento oftálmico roto y otro en el hipofisiario derecho no roto. Fue sometida a una craneotomía minipterional extradural más clipaje de aneurismas con oclusión completa y evolución favorable.
Conclusión: El conocimiento de nuevas técnicas microquirúrgicas en el manejo de aneurismas cerebrales complejos es crucial para obtener resultados satisfactorios, siendo el abordaje minipterional extradural un abordaje alternativo y clave para el tratamiento de estas lesiones, las cuales representan un desafío para el neurocirujano.
Palabras Clave: Aneurisma Intracraneal, Craneotomía, Circulación Colateral, Neurocirujanos (Fuente: DeCS Bireme)
INTRODUCTION
Complex aneurysms present various technical challenges due to their characteristics.1 They are a particular subtype of aneurysms in which the dimensions, location, presence of collateral flow, and prior endovascular or surgical treatment can exclude definitive endovascular or microsurgical treatment. 2
The operative planning of these aneurysms must be based on a balance between the risks and benefits for the patient, therefore neurosurgeons must be familiar with the concepts of cerebrovascular surgery, from transcranial approaches for clipping, endovascular treatments to bypass vascular techniques. 3, 12
The minipterional craniotomy (MPT) is part of the development of minimally invasive microsurgical techniques and technology.4 This approach allows obtaining corridors like the conventional pterional craniotomy, which provides an ideal approach for most intracranial aneurysms.5
This MPT approach associated with an extradural clinoidectomy, called by Figueiredo et al. The minipterional extradural approach (MiniPTEx), provides better exposure of the intracranial anatomical structures, according to the lesion we wish to treat.6
During the COVID19 pandemic, operating and hospital time is a determining factor in the primary outcome of a neurosurgical patient, being ideal to perform approaches that require less time with the same or better outcome than a classic approach.
In the neurosurgery department of our hospital, minimally invasive approaches are being carried out for the resolution of vascular pathologies. Therefore, in this case, report, the clipping of two complex aneurysms through a MiniPTEx approach is described.
CLINICAL CASE
History and examination: 33-year-old female patient, native and from Ayacucho with a history of embolization in 2019, of a left ophthalmic carotid aneurysm. She went to the emergency room with intermittent severe headache, nausea, and explosive vomiting. On physical examination: Patient awake, oriented, Glasgow scale: 15, without motor or sensory deficit, neck stiffness (+ / +++), isochoric and photoreactive pupils, decreased visual acuity in the right eye, Hunt-Hess scale 2.
Brain tomography showed subarachnoid hemorrhage (SAH), predominantly right, Fisher scale: II, with effacement of sulci and fissures. A 3D digital Panangiography was performed where 2 aneurysms were identified, a ruptured aneurysm of the right ophthalmic segment measuring 2.70 x 4.70 mm with a neck of 4.66 mm, saccular. A second unruptured right pituitary aneurysm measuring 4.40 x 3.81mm with a 5mm neck. (Figure 1)
 Fig 1. (A) 3D digital angiography of the right internal carotid artery (ICA) showing an aneurysm of the right ophthalmic segment and another of the pituitary. (B) Measurements of the right pituitary aneurysm. (C) 3D digital angiography of the right ICA showing an aneurysm in the ophthalmic segment and another in the pituitary segment. (D) Measurements of the aneurysm of the right ophthalmic segment. Fig 1. (A) 3D digital angiography of the right internal carotid artery (ICA) showing an aneurysm of the right ophthalmic segment and another of the pituitary. (B) Measurements of the right pituitary aneurysm. (C) 3D digital angiography of the right ICA showing an aneurysm in the ophthalmic segment and another in the pituitary segment. (D) Measurements of the aneurysm of the right ophthalmic segment. |
Microsurgical treatment: A minipterional craniotomy was performed with extradural clinoidectomy and clipping of 2 multiple complex aneurysms. There were no intraoperative complications.
The technique consisted of making a 6cm arcuate incision at the anterior limit of the scalp, 1cm above the zygomatic arch to the mid-pupillary line. (Figure 2A). The cutaneous flap was opened towards the anterior region, an interfacial approach was carried out with a scalpel, avoiding injury to the frontal branch of the facial nerve. (Figure 2B), then the interfacial fat was retracted anteriorly until the frontozygomatic arch was visible. The temporal fascia is cut through the superior temporal line towards the inferior, by means of subperiosteal dissection, a muscular flap is obtained that is displaced anteriorly. (Figure 2C).
The Burr hole was made with the help of a 4mm cutting bur behind the frontozygomatic process, then with a cutting blade the minipterional craniotomy was performed, taking as reference the superior temporal line and the pterion and stephanion craniometric points, achieving a craniotomy in diameter of 3 x 3cm. (Figure 2D, 2E)
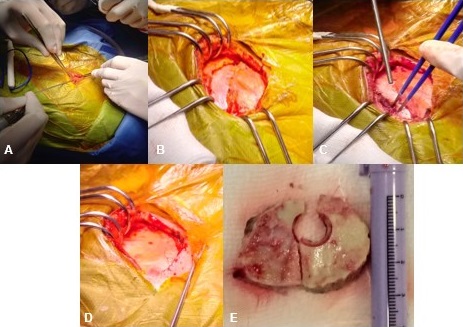 Fig 2. (A) Minipterional incision. (B) Interfacial dissection. (C) Interfacial vein coagulation (anatomical reference). (D) Exposure of bone area. (E) 3 x 3cm bone plate Fig 2. (A) Minipterional incision. (B) Interfacial dissection. (C) Interfacial vein coagulation (anatomical reference). (D) Exposure of bone area. (E) 3 x 3cm bone plate |
Then the sphenoid wing and orbital roof were drilled up to the lateral edge of the superior orbital fissure, achieving a greater area of vision. The mixed extradural anterior clinoidectomy was performed in a controlled and safe manner using a diamond bur and a fine gouge. Subsequently, the optic nerve is unroofed, with a 2mm diamond bur, under constant irrigation, and it is concluded with an incision of the falciform ligament for its release.
The dural opening was performed in a linear manner, retracting the folds to the lateral and medial direction, to expose the necessary work area. It started at the forward Silviano point forward. A subarachnoid exploration was performed with the opening of the carotid-ophthalmic and ophthalmic-oculomotor triangles, which allowed both aneurysms to be visualized. Clipping was done using 2 straight 7mm Yasargil clips.
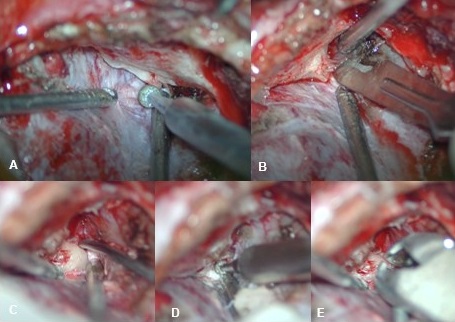 Fig 3. (A) Drilling of the sphenoid wing and orbital roof. (B) Release of the meningo-orbital band. (C) Exposure of the anterior clinoid process (PClA). (D) Drilling of the PClA attachment points. (E) PCA exeresis with a thin gouge. Fig 3. (A) Drilling of the sphenoid wing and orbital roof. (B) Release of the meningo-orbital band. (C) Exposure of the anterior clinoid process (PClA). (D) Drilling of the PClA attachment points. (E) PCA exeresis with a thin gouge. |
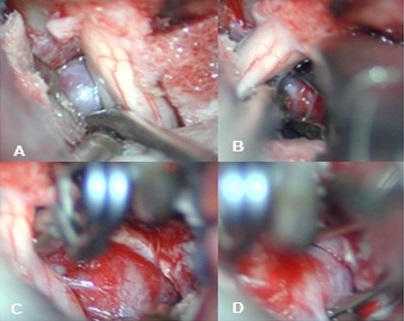 Fig 4. (A) Dome of the brain aneurysm of the right ophthalmic segment. (B-D) Clipping of cerebral aneurysm (D) Neck of right pituitary segment aneurysm. Fig 4. (A) Dome of the brain aneurysm of the right ophthalmic segment. (B-D) Clipping of cerebral aneurysm (D) Neck of right pituitary segment aneurysm. |
Clinical evolution: In the immediate postoperative period, the patient left awake, in Glasgow 15, with good clinical evolution and decreased right visual acuity that remained the same as that of the pre-surgical one. Postoperative brain tomography (CT) showed adequate clipping of the aneurysm and total closure of the neck of the aneurysm, without evidence of postoperative infarction.
DISCUSSION
Advances in microsurgical technique in neurovascular surgery have triggered modifications that have led to the minimization of craniotomies, designing optimal and safe management strategies for the complete occlusion of complex aneurysms. 7
The extradural minipterional (MiniPTEx) approach has been shown in multiple series to obtain excellent occlusal, functional, and aesthetic results. The MiniPTEx represents a small incision, reducing the degree of dissection of the skin, temporal muscle, and diameter of the craniotomy, in addition, the frontal sinus is not invaded, avoiding complications such as cerebrospinal fluid leakage and meningitis, greatly reducing hospital stay. 8,9
One of the challenges in the MiniPTEx is the area of work, especially when it comes to ruptured aneurysms that generate hydrocephalus and diffuse cerebral edema; this is solved with an adequate opening of the cisternae of the base (cisternostomy) and opening of the lamina terminalis, which reduces the phenomena of brain herniation and hydrocephalus.10,11.
In addition, sphenoid wing drift, interdural dissection, and anterior clinoidectomy are key steps in optimizing the use of this extradural corridor, allowing ideal maneuverability for secure clipping. 13
Aneurysms that involve the optic nerve result in visual alteration, therefore early decompression improves visual results.14 This release is feasible through the MiniPTEx approach, which allows wider surgical access to access lesions involving the base skull. 15
Microsurgical treatment was chosen over endovascular therapy in this case report, due to the type of supplies available in our hospital, in addition to having specialized personnel in vascular neurosurgery. However, the great advance that endovascular treatment has made in recent years is not downplayed.
In summary, the miniPTEX complies with the theoretical concept of transcranial approaches, which is to create a balance between maximum exposure, with a minimum degree of manipulation of the brain parenchyma.
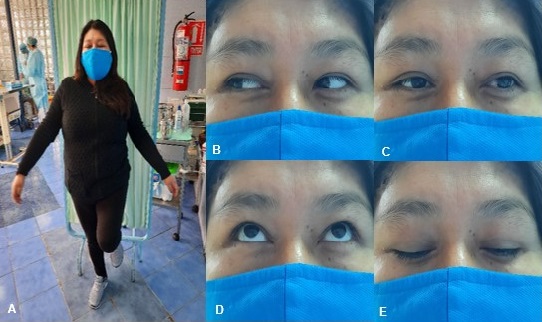 Fig 5. (A) Patient 30 days after surgery, without motor deficit. (B-E). Preserved eye movements (no oculomotor alteration) Fig 5. (A) Patient 30 days after surgery, without motor deficit. (B-E). Preserved eye movements (no oculomotor alteration) |
.
CONCLUSION
The treatment of certain types of complex aneurysms using microsurgical techniques such as the minipterional craniotomy offers us minimal trauma to the brain tissue, less bone removal, reduced surgical time, preservation of temporary function, and a better aesthetic result. This technique associated with an extradural clinoidectomy allows us to perform a safe and complete clipping, under the direct vision and control of adjacent neurovascular structures.
ETHICAL ASPECTS
The patient was informed about the publication of the case and the use of her photos, obtaining informed consent, attachments in the history under strict confidentiality.
REFERENCES
- Hacein-Bey L, Connolly ES Jr, Mayer SA, Young WL, Pile-Spellman J, Solomon RA. Complex intracranial aneurysms: combined operative and endovascular approaches. Neurosurgery. 1998 Dec;43(6):1304-12; discussion 1312-3.
- Hanel, R. A., & Spetzler, R. F. (2008). Surgical Treatment of Complex Intracranial Aneurysms. Neurosurgery, 62(Supplement 3), SHC1289–SHC1299.
- Figueiredo EG, Teixeira MJ, Spetzler RF, et al. Clinical and surgical experience with the minipterional craniotomy. Neurosurgery 2014;75: E324–5.
- Vishteh AG, Marciano FF, David CA, Baskin JJ, Spetzler RF. The pterional approach. Oper Tech Neurosurg. 1998;1(1):39-49.
- Caplan JM, Papadimitriou K, Yang W, et al. The minipterional craniotomy for anterior circulation aneurysms: initial experience with 72 patients. Neurosurgery 2014;2: 200–6 [discussion 206–7].
- Campero A, Londoño-Herrera D, Ajler P. Abordaje pterional. Rev argent neuroc. 2015. Vol 29(1): 49-53.
- Figueiredo EG, Welling LC, Preul MC, et al. Surgical experience of minipterional craniotomy with 102 ruptured and unruptured anterior circulation aneurysms. J Clin Neurosci. 2016; 27:34-39.
- Mura J, Perales I, Rabelo NN, Martínez-Pérez R, Poblete T, González-Llanos F, et al. Extradural minipterional approach: Evolving indications of the minipterional craniotomy. Surg Neurol Int 2020; 11:109.
- Mishra, S., Leão, B. y Rosito, DM (2017). Clinoidectomía anterior extradural: matices técnicos desde la perspectiva del alumno. Revista asiática de neurocirugía, 12 (2), 189-193.
- Pescatori L, Tropeano MP, Santoro A. Complex Aneurysm: The Unpredictable Pathological Entity. Acta Neurochir Suppl. 2018; 129:61-70.
- Chiarullo M, Mura J, Rubino P, Rabelo NN, Martinez-Perez R, Figueiredo EG, Rhoton A. Technical Description of Minimally Invasive Extradural Anterior Clinoidectomy and Optic Nerve Decompression. Study of Feasibility and Proof of Concept. World Neurosurg. 2019 Sep;129: e502-e513.
- Gallardo FC, Bustamante JL, Martin C, Targa Garcia AA, Feldman SE, Pastor F, Orellana MC, Rubino PA, Quilis Quesada V. Intra- and extradural anterior clinoidectomy: anatomy review and surgical technique step by step. Surg Radiol Anat. 2021 Jan 25.
- Alkhalili, K. A., Hannallah, J. R., Alshyal, G. H., Nageeb, M. M., & Abdel Aziz, K. M. (2017). The minipterional approach for ruptured and unruptured anterior circulation aneurysms: Our initial experience. Asian journal of neurosurgery, 12(3), 466–474.
- Cabrilo, I., Schaller, K., & Bijlenga, P. (2015). How Mini Can Minipterional Craniotomies Get? Neurosurgery, 76(1), E101–E102.
- Martinez-Perez R, Tsimpas A, Joswig H, Hernandez-Alvarez V, Mura J. Extradural minipterional approach for giant intracranial aneurysms. Surg Neurol Int. 2020 Nov 11; 11:382
__________________________________________________________
Disclosures
The authors report no conflict of interest concerning the materials or methods used in this study or the findings specified in this paper.
Authors' Contributions
Conception and design: All authors. Drafting the article: Salazar C. Critically revising the article: Díaz, Rojas, Gaitán, Lúcar. Reviewed submitted version of manuscript: Salazar. Approved the final version of the manuscript on behalf of all authors: Salazar.
Correspondencia
Cristian Eugenio Salazar Campos. Department of Neurosurgery of the “Luis N. Saenz” PNP Hospital Complex. 2650 Brazil Avenue. Jesús María. Lima, Peru. E-mail: cristiansc92@gmail.com